Magnesium and PMT: an effective remedy or just a myth?

Magnesium deficiency can play a significant role in a number of different clinical conditions regarding women’s health, and above all in premenstrual tension (PMT). In fact numerous studies have shown a positive correlation between taking magnesium and the alleviation or prevention of symptoms, both physical and mental, associated with the premenstrual phase, thus suggesting that magnesium supplements can represent a useful choice for women suffering from this problem.
As already dealt with in detail in our article on the functions of magnesium and its importance for our health, this mineral is essential for our health, as it contributes to:
- A normal energy-yielding metabolism;
- Well-being of the nervous system;
- Reducing fatigue and facilitating muscle relaxation;
- normal psychological functions.
Let’s now look into the correlation between magnesium and PMT in more detail.
The phases of the menstrual cycle: when does PMT start?
The menstrual cycle is a process controlled by female hormones that enable the formation of the egg and fertilisation by the spermatozoa; if the egg is not fertilised, it is destroyed, with the consequent loss of blood, known now as menstruation.
This cycle is considered regular when it has an average duration of 28 days: in general, it can range from 24 to 32 days, and blood loss may be light or heavy, lasting between 3 and 7 days.
When the menstrual flow is heavy, this may lead to iron deficiency; in this case, the values of this mineral need to be monitored, above all if blood test results show low levels. As we know only too well, menstruation during the menstrual cycle is often accompanied by other unpleasant symptoms, with pain in the form of abdominal cramps and tension: This condition is identified in medicine with the term dysmenorrhea and it is quite frequent (in mild or acute forms) above all under the age of 20.
The menstrual cycle is divided into three distinct phases:
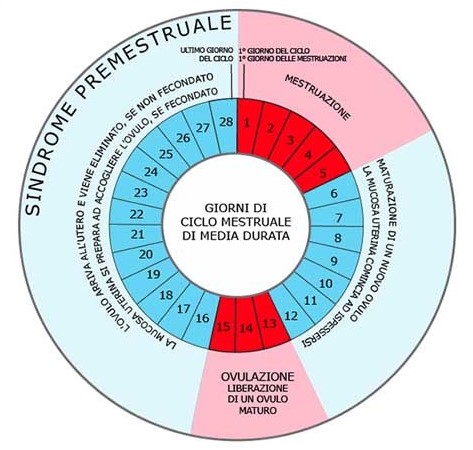
- Follicular or proliferative phase: The follicular phase starts on the first day of the menstrual flow, which corresponds to the first day of the cycle and lasts 7-10 days. In this phase the Follicle Stimulating Hormone (FSH) is formed, increasing the production of oestrogen, which causes the endometrium walls to thicken (the inner mucous membrane lining of the uterus), so that it can receive the fertilised egg.
- Ovulatory phase: This is a short phase (around three days) in which the mature egg is formed and released from the follicle. What remains transforms into a “temporary” gland, known as corpus luteum, which produces progesterone, the hormone that has the task of allowing fertilisation and useful for maintaining the pregnancy.
- Luteal phase: In this last phase of the cycle, a favourable environment is created to allow fertilisation of the egg by the spermatozoa; if this does not occur, the egg is re-absorbed by the endometrium and the corpus luteum is destroyed, causing a reduction of progesterone, with the consequent shedding of the endometrium and the menstrual flow.
Rate of PMT among women: the most common symptoms
Premenstrual tension is a very common disorder, affecting above all girls and young women. PMT is a condition with both physical and mental symptoms, that appear during the luteal phase of the menstrual cycle, and therefore at around 10 days before the actual menstrual flow.

In all, it affects 80-90% of women of childbearing age, and, among these, 30-40% require special treatment to deal with the symptoms. Although the symptoms are subjective and can vary greatly from woman to woman, the most commonly reported include irritability, headache, anxiety and agitation, insomnia, difficulty concentrating, lack of energy, melancholy and fatigue. Added to these are feeling bloated, feelings of heaviness and tension in the lower abdomen in all, these are symptoms which if attributable to premenstrual tension are not alarming in themselves but can obviously cause discomfort and malaise for several days.
How does magnesium act on PMT?
A number of studies confirm that women suffering from PMT show a deficiency of magnesium, caused by an increase in the production of some hormones, such as progesterone, which leads to a high urinary excretion of this mineral.
On the other hand, other studies show that women treated with magnesium from the first day after ovulation through to the start of the cycle have improved symptoms related to PMT; in fact, magnesium, among its various functions, aids and intervenes in the synthesis of serotonin, the “good mood” hormone, essential above all at moments when women feel agitated, down and/or anxious.
Furthermore, magnesium is necessary to stabilise and control the activity of Adenosine triphosphate (ATP), the molecule responsible for supplying energy to the cells of the body; in particular, magnesium contributes to the use of ATP in muscle contractions, a very important factor to consider when we talk of physical fatigue linked to PMT.
Meanwhile, as regards headaches, some studies have shown a close link with low levels of magnesium. In fact, this deficiency causes an increase in platelet aggregation with high levels of serotonin, which leads to vasoconstriction, the trigger factor for headaches.
However, this isn’t to say that magnesium is a painkiller and should never be intended as such. So, we need to know how to take it correctly so that it is an effective remedy against premenstrual tension.
How and when to take magnesium to alleviate or prevent symptoms of PMT
As we have seen, magnesium is useful in preventing and reducing symptoms of PMT, and supplements are recommended during the luteal phase, in other words from the 16ᵗʰ day of the cycle.
The first recommendation is to carefully choose food that has a higher content of magnesium. Food rich in this mineral are green-leafed vegetables, such as spinach, walnuts and wholewheat cereals; a smaller percentage is also found in fruit, meat, fish and dairy products. However, take care when cooking: Even a short cooking time significantly reduces the content of magnesium and in general of vitamins and nutrients in food.
Hydration is also essential. Indeed 10% of the required daily intake of magnesium comes from the water we drink (so-called “hard” water is the type most rich in mineral salts).
Let’s not forget also that the Recommended Dietary Allowance (RDA) of magnesium for women varies with age:
| 9-13 years | 240 mg/die |
| 14-18 years | 360 mg/die |
| 19 years and older | 320 mg/die |
Table 1: Recommended Dietary Allowance of magnesium for women according to age
When the intake of this mineral is not sufficient to meet the demands of our body, normal diet can be combined with specific nutritional magnesium supplements.
However, at times it is difficult to choose the supplement most suited to your needs. No all supplements on sale contain the same type of magnesium and it is here that it’s essential to know the difference. Magnesium can be found in the form of various salts:
- Inorganic magnesium salts (e.g., magnesium oxide);
- Organic magnesium salts (e.g., magnesium pidolate);
- Chelated magnesium salts (e.g., magnesium bisglycinate).
Among these, magnesium oxide (MgO) is undoubtedly the one with the highest content of elementary magnesium, although absorption by the body is very limited.
To overcome this limitation, UltraMag®, a supplement based on magnesium oxide, uses Sucrosomial® technology. In this case the mineral is conveyed in a matrix of phospholipids and saccharic esters of the fatty acids, which enables high absorption of magnesium and optimal gastrointestinal tolerability. The dose of magnesium oxide in UltraMag® is 375 mg, which corresponds to 100% of the Dietary reference intake (DRI). For this reason, we recommend taking one sachet a day dissolved in a glass of water, at any time of the day.
BIBLIOGRAPHY:
- Banerjee S., Jones S., Magnesium as an Alternative or Adjunct to Opioids for Migraine and Chronic Pain: A Review of the Clinical Effectiveness and Guidelines; Canadian Agency for Drugs and technologies in Health: Ottawa, On, Canada, 2017.
- Rosenstein D.L., Elin R.J., Hosseini J.M., Grover G., Rubinow D.R., Magnesium measures across the menstrual cycle in premenstrual syndrome. Biol Psychiatry. 1994 Apr 15;35.
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine (IOM). Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academies Press: Washington, DC, USA, 1997.
- Mauskop A., Altura B.T., Cracco R.Q., Altura B.M., Intravenous magnesium sulfate rapidly alleviates headaches of various types. Headache 1996, 36, 154–160.
- Parazzini F., Di Martino M., Pellegrino P., Magnesium in the gynecological practice: a literature review. Magnes Res. 2017 Feb 1;30(1):1-7.